Pallister–Hall syndrome
This article needs additional citations for verification. (August 2020) |
| Pallister–Hall syndrome (PHS) | |
|---|---|
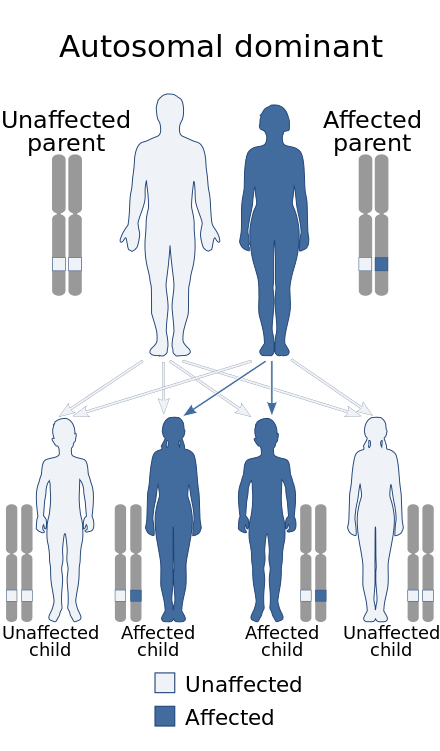 | |
| Pallister–Hall syndrome is inherited in an autosomal dominant pattern. | |
| Specialty | Medical genetics |
| Named after |
|
Pallister–Hall syndrome (PHS) is a rare genetic disorder that affects various body systems.[1] The main features are a non-cancerous mass on the hypothalamus (hypothalamic hamartoma) and extra digits (polydactylism). The prevalence of Pallister-Hall Syndrome is unknown; about 100 cases have been reported in publication.[2]
History
[edit]The syndrome was originally described by American and Canadian geneticists Philip Pallister and Judith Hall in their research of newborn deaths due to pituitary failure.[3] Subsequent discovery of living children and adults expanded the understanding of the syndrome and established the transmission pattern within families.[4]
Presentation
[edit]The main characteristics of the syndrome are extra fingers and/or toes (polydactyly), with the skin between some fingers or toes potentially fused or "webbed" (cutaneous syndactyly), and a benign mass or lesion in the brain called a hypothalamic hamartoma.[5] This benign tumor may not cause any medical problems; however, some hypothalamic hamartomas lead to seizures or hormone abnormalities. Other features of Pallister–Hall syndrome include a split opening of the airway called bifid epiglottis, laryngeal cleft, blockage of the anal opening (imperforate anus), and kidney abnormalities. Signs and symptoms of this disorder vary from mild to severe.
Seizures
[edit]The most common type of seizure from this disorder of that occur is known as gelastic epilepsy or "laughing" seizures. Seizures may begin at any age but usually before three or four years of age. The seizures usually start with laughter described as being "hollow" or "empty" and unpleasant. The laughter occurs suddenly for no obvious reason and is often out of place. Other traditional seizure types such as tonic-clonic and absence seizures may also develop due to temporal lobe epilepsy.[6] People with Pallister-Hall may experience less severe seizures than people with a hypothalamic hamartoma only.[7]
Transmission
[edit]Pallister-Hall Syndrome occurs due to a mutation in the GLI3 gene that overrides normal genetic development.[8] Before birth the GLI3 gene delivers directions for protein creation that turns on or off development of cells that produce organs and tissues. The abnormal GLI3 gene is shortened and can only turn off targeted genes.
Pallister-Hall Syndrome is transmitted in an autosomal dominant pattern. One copy of the altered gene in each cell is sufficient to cause the disorder. Thus, the child of one parent with PHS would have a 50% chance of inheriting the gene that causes the syndrome.[9] Some cases can still result from new mutations in the gene and occur in people with no history of the disorder in their family.
Diagnosis
[edit]Central characteristics of the disorder include polydactyly (extra digits on limbs) with possible cutaneous syndactyly (fusion or webbed skin between some fingers or toes) and a hypothalamic hamartoma, a rare brain lesion on the hypothalamus that is present at birth. While the mass may occur unrelatedly, the presence of polysyndactyly warrants investigation for PHS.[10] Currently, clinical diagnosis is through a brain MRI and genetic sequencing for GLI 13 gene, which is known to cause Pallister-Hall Syndrome, as well as Greig cephalopolysyndactyly syndrome. Genetic testing can find and identify the corresponding disorder.[11]
Treatment
[edit]Treatment is limited to physical signs and symptoms of the hypothalamic hamartoma. Surgery may be required at birth to fix imperforate anus and address endocrine abnormalities. Selective removal of extra digits may occur in early childhood. Parents and medical practitioners should monitor for signs of endocrine disruption in sleep, eating, or hormonal issues, such as precocious puberty caused by the hypothalamic hamartoma.
Seizures may be treated with anticonvulsants. However, gelastic seizures are often intractable and may not benefit from such therapy.[12] Resection of the hypothalamic hamartoma has improved seizure control and hypothalamic function in some patients.[13]
References
[edit]- ^ "Pallister-Hall syndrome | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program".
- ^ Shourick, Jason; Wack, Maxime; Jannot, Anne-Sophie (2021-03-20). "Assessing rare diseases prevalence using literature quantification". Orphanet Journal of Rare Diseases. 16 (1): 139. doi:10.1186/s13023-020-01639-7. ISSN 1750-1172. PMC 7980535. PMID 33743790.
- ^ Hall JG, Pallister PD, Clarren SK, et al. (1980). "Congenital hypothalamic hamartoblastoma, hypopituitarism, imperforate anus and postaxial polydactyly--a new syndrome? Part I: clinical, causal, and pathogenetic considerations". Am. J. Med. Genet. 7 (1): 47–74. doi:10.1002/ajmg.1320070110. PMID 7211952.
- ^ Biesecker, L. G.; Topf, K.; Graham, J. M. (September 1994). "Familial Pallister-Hall syndrome". Journal of Medical Genetics. 31 (9): 740. doi:10.1136/jmg.31.9.740-a. ISSN 0022-2593. PMC 1050091. PMID 7880273.
- ^ Biesecker, L. G.; Abbott, M.; Allen, J.; Clericuzio, C.; Feuillan, P.; Graham, J. M.; Hall, J.; Kang, S.; Olney, A. H.; Lefton, D.; Neri, G.; Peters, K.; Verloes, A. (October 1996). "Report from the workshop on Pallister-Hall syndrome and related phenotypes". American Journal of Medical Genetics. 65 (1): 76–81. doi:10.1002/(SICI)1096-8628(19961002)65:1<76::AID-AJMG12>3.0.CO;2-O. ISSN 0148-7299. PMID 8914745.
- ^ Kremer, Stéphane; Minotti, Lorella; Thiriaux, Anne; Grand, Sylvie; Satre, Véronique; Le Bas, Jean-François; Kahane, Philippe (March 2003). "Epilepsy and hypothalamic hamartoma: look at the hand Pallister-Hall syndrome". Epileptic Disorders: International Epilepsy Journal with Videotape. 5 (1): 27–30. ISSN 1294-9361. PMID 12773293.
- ^ Boudreau, Eilis A.; Liow, Kore; Frattali, Carol M.; Wiggs, Edith; Turner, Joyce T.; Feuillan, Penelope; Sato, Susumu; Patsalides, Athos; Patronas, Nicholas; Biesecker, Leslie G.; Theodore, William H. (January 2005). "Hypothalamic hamartomas and seizures: distinct natural history of isolated and Pallister-Hall syndrome cases". Epilepsia. 46 (1): 42–47. doi:10.1111/j.0013-9580.2005.68303.x. ISSN 0013-9580. PMID 15660767. S2CID 31163166.
- ^ Kang, S.; Graham, J. M.; Olney, A. H.; Biesecker, L. G. (March 1997). "GLI3 frameshift mutations cause autosomal dominant Pallister-Hall syndrome". Nature Genetics. 15 (3): 266–268. doi:10.1038/ng0397-266. ISSN 1061-4036. PMID 9054938. S2CID 31776794.
- ^ "Pallister-Hall syndrome - About the Disease - Genetic and Rare Diseases Information Center". rarediseases.info.nih.gov. Retrieved 2023-03-20.
- ^ Biesecker, Leslie G. (1993), Adam, Margaret P.; Mirzaa, Ghayda M.; Pagon, Roberta A.; Wallace, Stephanie E. (eds.), "GLI3-Related Pallister-Hall Syndrome", GeneReviews®, Seattle (WA): University of Washington, Seattle, PMID 20301638, retrieved 2023-03-20
- ^ Johnston, Jennifer J.; Olivos-Glander, Isabelle; Killoran, Christina; Elson, Emma; Turner, Joyce T.; Peters, Kathryn F.; Abbott, Margaret H.; Aughton, David J.; Aylsworth, Arthur S.; Bamshad, Michael J.; Booth, Carol; Curry, Cynthia J.; David, Albert; Dinulos, Mary Beth; Flannery, David B. (April 2005). "Molecular and clinical analyses of Greig cephalopolysyndactyly and Pallister-Hall syndromes: robust phenotype prediction from the type and position of GLI3 mutations". American Journal of Human Genetics. 76 (4): 609–622. doi:10.1086/429346. ISSN 0002-9297. PMC 1199298. PMID 15739154.
- ^ Helen Cross, J.; Spoudeas, Helen (June 2017). "Medical management and antiepileptic drugs in hypothalamic hamartoma". Epilepsia. 58 (Suppl 2): 16–21. doi:10.1111/epi.13758. ISSN 1528-1167. PMID 28591485. S2CID 205119031.
- ^ Bourdillon, Pierre; Ferrand-Sorbet, S.; Apra, C.; Chipaux, M.; Raffo, E.; Rosenberg, S.; Bulteau, C.; Dorison, N.; Bekaert, O.; Dinkelacker, V.; Le Guérinel, C.; Fohlen, M.; Dorfmüller, G. (April 2021). "Surgical treatment of hypothalamic hamartomas". Neurosurgical Review. 44 (2): 753–762. doi:10.1007/s10143-020-01298-z. ISSN 1437-2320. PMID 32318922. S2CID 216049240.
- Pallister–Hall syndrome at NLM Genetics Home Reference