Spondyloenchondrodysplasia
| Spondyloenchondrodysplasia | |
|---|---|
| Other names | Spondyloenchondrodysplasia with immune dysregulation, Combined immunodeficiency with autoimmunity and spondylometaphyseal dysplasia, Roifman immunoskeletal syndrome, SPENCD (abbr.), SEM (abbr.), Spondylometaphyseal dysplasia with enchondromatous changes, Spondyloenchondromatosis[1][2] |
 | |
| Specialty | Medical genetics |
| Symptoms | Vary widely among patients |
| Usual onset | Birth–Childhood |
| Duration | Lifelong |
| Causes | Genetic mutation |
| Frequency | rare |
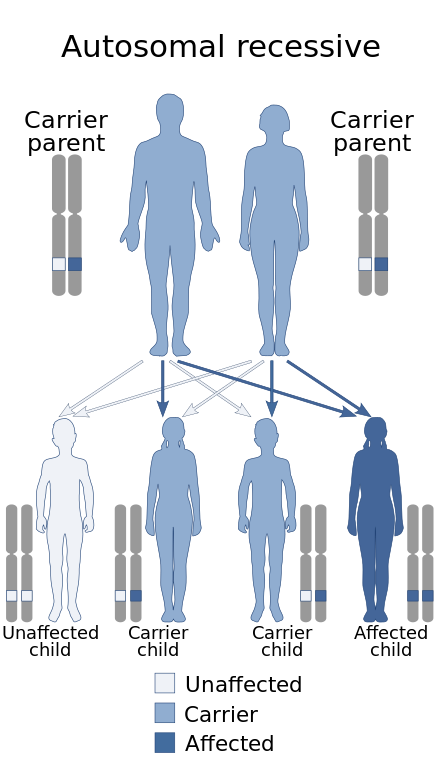
Spondyloenchondrodysplasia is the medical term for a rare spectrum of symptoms that are inherited following an autosomal recessive inheritance pattern. Skeletal anomalies (including abnormal bone growths) are the usual symptoms of the disorder, although its phenotypical nature is highly variable among patients with the condition, including symptoms such as muscle spasticity or thrombocytopenia purpura.[3] It is a type of immunoosseous dysplasia.[4]
Signs and symptoms
[edit]Heterogeneity in this disorder causes the phenotype and severity of the symptoms caused by the disorder to vary widely among patients with the condition, these subsets of symptoms include those affecting the immune system (causing autoimmune diseases and resulting in the disruption of other systems such as the hematological one), the neurological system, and many more.[5][6]
Skeletal symptoms
[edit]This condition primarily constitutes skeletal anomalies. [citation needed]
These include metaphyseal dysplasia, platyspondyly and the presence of lesions located in the long bones and the spinal vertebrae, and enchondroma. [citation needed]
Cartilage symptoms
[edit]This subset of symptoms affecting the cartilage. [citation needed]
They include the presence of enchondroma and the failure of cartilage to turn into bone in some parts of the body. [citation needed]
Immune symptoms
[edit]This subset of symptoms primarily affects the immune system (immunodeficiency) and also causes autoimmune diseases, which indirectly affect other systems of the body. [citation needed]
These include thrombocytopenia, rheumatoid arthritis, systemic lupus erythematosus, recurrent respiratory infections and fevers, hemolytic anemia, and hypothyroidism. [citation needed]
Neurological symptoms
[edit]This subset of symptoms affects the central nervous system. [citation needed]
These include ataxia, muscle spasticity, intellectual disabilities, and cerebral calcification. [citation needed]
Other findings
[edit]Other features that may be found in patients with this condition include short stature, dental eruption delay, dental malocclusion, vitiligo, seizures, pectus carinatum, kyphosis, kyphoscoliosis, ventriculomegaly, vasculitis, Raynaud's phenomenon, pain affecting the lower limbs, chronic headaches, chronic kidney disease, cranio-facial dysmorphisms, hypoplasia of the iliac bones, lupus nephritis, arthralgia, arthritis, hypocomplementemia, low to absent TRAP enzyme in serum, high levels of interferon-alpha in the serum, and an over-expression of interferon-stimulated genes.[7][6][8][9]
Rare symptoms include intellectual disability, developmental delay, progressive spastic quadriplegia, temporomandibular joint pain, hepatosplenomegaly, and spina bifida.[7][10][8][11]
Complications
[edit]Premature death may result from the immunodeficiency and/or autoimmunity associated with this condition.[12][13]
Genetics
[edit]
This condition is caused by autosomal recessive loss-of-function mutations in the ACP5 gene, located in chromosome 19. This gene encodes an iron-containing enzyme known as tartrate-resistant acid phosphatase,[14][7] which regulates a protein known as osteopontin. Immune system cells is among the many systems this protein plays a role in.[15][16][17]
Individuals with this condition have over-active osteopontin protein due to the fact that the TRAP enzyme is unable of inactivating it. The impaired TRAP enzyme is a result of the ACP5 mutation involved with the condition. Osteopontin hyperactivity in patients with spondyloenchondroplasia results in over-produced interferon 1 protein, a bone breakdown process that is longer than usual and an unusually over-active immune system. Both of these altered mechanisms cause skeletal anomalies, autoimmunity, and immunodeficiency as a result.[15][18]
In rare cases, spondyloenchondroplasia may be inherited in an autosomal dominant manner.[19]
Diagnosis
[edit]There are various ways of diagnosing spondyloenchondroplasia:
Physical examination
[edit]Description of physical findings in patients with spondyloenchondroplasia is essential for a proper diagnosis. The most common physical finding is short stature. [citation needed]
The four patients described by Frydman et al. (1986) had a stature that was three standard deviations below average.[20]
The two Turkish siblings with the condition reported by De Bruin et al. (2016) had extreme short stature.[21]
Radiographs
[edit]All cases in the medical literature of spondyloenchondroplasia have included a description of the adiological anomalies shown by patients with the condition which were found on radiographs. [citation needed]
A 5-year-old Indian boy reported by Kulkarni et al. (2007) had anomalies of his metaphyses and vertebrae bones which were visible under X-ray. These are common skeletal features shared by patients with spondyloenchondroplasia.[22]
Two brothers born of a consanguineous first-cousin Iraqi Jewish union had enchondromatosis which was visible under radiographs.[23]
One of the four patients analyzed by Menger et al. (1989) had vertebral anomalies that were visible on radiographs. Said patient was the product of father-daughter incest.[24]
Uhlmann et al. (1998) found spinal anomalies, flattened bones, and tubular enchondromas in 2 boys with the condition which were visible on radiographs.[25]
Genetic testing
[edit]Genetic testing methods are essential for a diagnosis of spondyloenchondroplasia, said diagnostic methods must detect a mutation in the ACP5 gene of the patient with the condition. [citation needed]
Girschick et al. (2015) found a missense mutation and a 1 base pair duplication in the ACP5 gene of a 9-year-old girl with the condition. Both mutations were homozygous. Her parents were heterozygous for only one of the mutations.[26]
Genetic testing done on the 5-year-old Indian boy reported by Kulkarni et al. (2007) showed a 5-kb deletion in his ACP5 gene, present in a homozygous state.[22]
Lausch et al. (2011) found a mutation in the ACP5 gene of 5 families with the condition after performing targeted genetic sequencing (at ACP5) on them.[27]
Sema et al. (2021) found a homozygous mutation (c.155A > C) in the ACP5 gene of a 19-year-old Turkish man with the condition.[28]
Among the many patients in the study, Briggs et al. (2011) found a homozygous C>T substitution in exon 4 of the ACP5 gene of two Turkish siblings of the opposite sex which lead to a threonine to isoleucine substitution at amino acid position 89 of the gene. The mutation was found thanks to genetic sequencing.[29]
Laboratory studies
[edit]Various biochemical anomalies can be found in patients with the condition through laboratory studies. [citation needed]
The affected 9-year-old girl and her unaffected parents reported by Girschick et al. (2015) had levels of TRAP enzyme lower than average in their blood.[26]
An Egyptian girl reported by Briggs et al. (2011) was found to have antinuclear antibody, anti-dsDNA antibody titers, microglobulinemia, and hypogammaglobulinemia.[29]
Hermann et al. reported a 9-year-old German girl with the condition, laboratory tests done on her showed high levels of interferon-α in her cerebrospinal fluid and serum, abnormal results from liver function tests, IcG, decreased levels of CD4+ cells, B cells, and natural killer cells, and the presence of autoantibodies.[26]
Differential diagnosis
[edit]Conditions that might be confused with spondyloenchodroplasia include:[30][31][32][33]
- Metachondromatosis, a rare autosomal dominant genetic disorder characterized by metaphyseal enchondromas and exostoses of the hands and feet.[34]
- Genochondromatosis, a very rare autosomal dominant genetic disorder characterized by humeral and femural enchondromas which don't cause short stature.[34]
- Dysspondylochondromatosis[33]
- Pseudoachondroplasia, a rare autosomal dominant genetic disorder characterized by disproportionate short stature, waddling gait, ligamentous laxity, short fingers and various other radiological anomalies, including (but not limited to) abnormally late-onset epiphyseal ossification and lumbar lordosis.[35]
Treatment
[edit]Although no standard management strategy for spondyloenchondroplasia exists, there have been various treatment methods done on patients with the condition reported in the medical literature.
Growth hormone therapy
[edit]The 21-year-old sister of the proband reported by Tuyzus et al. (2004) had undergone growth hormone therapy 12 years prior to the study in order to treat her severely short stature.[36]
Takanori et al. (2017) described successful treatment for spondyloenchondroplasia-associated short stature with growth hormone therapy on a child with the condition.[17]
Methylprednisolone pulse therapy
[edit]The German girl reported by Hermann et al. underwent methylprednisolone pulse therapy, which later lessened the severity of her muscle spasticity.[26]
Mycophenolate mofetil
[edit]The aforementioned German girl was prescribed with a 250 mg daily dose of mycophenolate mofetil which later improved her motor function and her blood platelet count.[26]
Prednisolone
[edit]After a hospitalization at the age of 5 years old as a result of a sudden onset of clinical symptoms including bloody diarrhea, a high fever, pneumonia, and polyarthritis, the aforementioned girl was prescribed a 20 mg daily dose of prednisolone, which later improved her symptoms.[26]
Baricitinib
[edit]Masaki et al. (2020) described an 8-year-old girl with Turner syndrome (46, X, idic(X) (p11.2) [55%]/45, XX [45%] karyotype) and spondyloenchondroplasia. She was treated with growth hormone therapy at first but it barely treated her short stature. She was then given a prescription for a daily dose of prednisolone and mycophenolate mofetil, and while said prescription improved some of her symptoms, her recurrent fevers and headaches didn't stop, she was then prescribed a 2–4 mg daily dose of baricitinib, the latter medication significantly improved her serum ferritin levels and her IFN score. She faced no side effects from this medication.[37]
Prevalence
[edit]According to OMIM, only around 30–40 cases have been described in the medical literature.[38]
History
[edit]Discovery of the disorder
[edit]This condition was first described in 2003 by Roifman et al., the amount of patients they described was four.[39]
The first two patients were a pair of siblings of the opposite sex (brother and sister) born to consanguineous first-cousin Portuguese parents. The sister was noted to have suffered from various health complications, including recurrent infections (primarily those affecting the respiratory system), chronic restrictive lung disease, idiopathic thrombocytopenic purpura, and an enlarged thyroid accompanied by hypothyroidism. Her thrombocytopenic purpura didn't resolve with the use of either prednisone or intravenous immunoglobulin, but it did after a splenectomy was performed on her. The younger brother had presumably died, and had suffered from various ailments like her sister, including recurrent respiratory infections, campylobacter enteritis, idiopathic thrombocytopenic purpura, and encephalitis, the latter of which caused his aforementioned death.[39]
The other 2 patients constituted of a 5-year-old boy who suffered from recurrent respiratory infections, hemorrhagic chickenpox, and idiopathic thrombocytopenic purpura. The fourth and final case was that of a 10-year-old-boy who had recurrent infections, Crohn's disease, and hypothyroidism.[39]
Discovery of the disorder's molecular basis
[edit]The gene involved in spondyloenchondroplasia was found in 2011 by Briggs et al., their study included 10 participants with the condition from 8 families worldwide. Homozygosity mapping in the patients linked the 19p13 region of the 19th chromosome to the disorder. Further genetic analysis showed mutations in the ACP5 gene. Of these 10 patients, half were born to consanguineous parents and half were not, although genetic analysis on one pair of seemingly unrelated parents gave the possibility that they were distantly related.[29]
See also
[edit]- Achondroplasia
- Achondrogenesis
- Autosomal recessive multiple epiphyseal dysplasia
- Osteochondrodysplasia
References
[edit]- ^ "UniProt". www.uniprot.org. Retrieved 2022-10-23.
- ^ "Spondyloenchondrodysplasia with immune dysregulation". NORD (National Organization for Rare Disorders). Retrieved 2022-10-23.
- ^ "Orphanet: Spondyloenchondrodysplasia". www.orpha.net. Retrieved 2022-10-23.
- ^ "Spondyloenchondrodysplasia with immune dysregulation (Concept Id: C1842763) - MedGen - NCBI". www.ncbi.nlm.nih.gov. Retrieved 2022-10-23.
- ^ "Spondyloenchondrodysplasia with immune dysregulation: MedlinePlus Genetics". medlineplus.gov. Retrieved 2022-10-23.
- ^ a b "Spondyloenchondrodysplasia with immune dysregulation - About the Disease - Genetic and Rare Diseases Information Center". rarediseases.info.nih.gov. Retrieved 2022-10-23.
- ^ a b c "Kegg Disease: Spondyloenchondrodysplasia with immune dysregulation (SPENCDI)". www.genome.jp. Retrieved 2022-10-23.
- ^ a b Hong SW, Huh KH, Lee JK, Kang JH (December 2018). "Craniofacial anomalies associated with spondyloenchondrodysplasia: Two case reports". Medicine. 97 (50): e13644. doi:10.1097/MD.0000000000013644. PMC 6320149. PMID 30558059. S2CID 56176080.
- ^ Bilginer Y, Düzova A, Topaloğlu R, Batu ED, Boduroğlu K, Güçer Ş, et al. (June 2016). "Three cases of spondyloenchondrodysplasia (SPENCD) with systemic lupus erythematosus: a case series and review of the literature". Lupus. 25 (7): 760–765. doi:10.1177/0961203316629000. PMID 26854080. S2CID 34645935.
- ^ Bissonnette B, Luginbuehl I, Engelhardt T (2019). "Spondyloenchondrodysplasia". Syndromes: Rapid Recognition and Perioperative Implications (2nd ed.). New York, NY: McGraw-Hill Education. Retrieved 2022-10-23.
- ^ Bortoli AF, de Borba Capaverde V, Acco FS, Kiss A, Flores JA, Rosa RF (2020). "Hallazgos radiológicos en un niño con espondiloencondrodisplasia". Revista argentina de radiología. 84 (2): 71–74.
- ^ Briggs TA, Rice GI, Adib N, Ades L, Barete S, Baskar K, et al. (April 2016). "Spondyloenchondrodysplasia Due to Mutations in ACP5: A Comprehensive Survey". Journal of Clinical Immunology. 36 (3): 220–234. doi:10.1007/s10875-016-0252-y. PMC 4792361. PMID 26951490.
- ^ "Spondyloenchondrodysplasia with Immune Dysregulation (SPENCDI)". www.malacards.org. Retrieved 2022-10-23.
- ^ "ACP5 Gene - GeneCards | PPA5 Protein | PPA5 Antibody". www.genecards.org. Retrieved 2022-10-23.
- ^ a b "ACP5 gene: MedlinePlus Genetics". medlineplus.gov. Retrieved 2022-10-23.
- ^ Ramesh J, Parthasarathy LK, Janckila AJ, Begum F, Murugan R, Murthy BP, et al. (2020). "Characterisation of ACP5 missense mutations encoding tartrate-resistant acid phosphatase associated with spondyloenchondrodysplasia". PLOS ONE. 15 (3): e0230052. Bibcode:2020PLoSO..1530052R. doi:10.1371/journal.pone.0230052. PMC 7098635. PMID 32214327.
- ^ a b Utsumi T, Okada S, Izawa K, Honda Y, Nishimura G, Nishikomori R, et al. (2017). "A Case with Spondyloenchondrodysplasia Treated with Growth Hormone". Frontiers in Endocrinology. 8: 157. doi:10.3389/fendo.2017.00157. PMC 5502255. PMID 28740483.
- ^ Bağlan E, Özdel S, Güngör T, Karakuş R, Bağrıaçık EÜ, Yücel AA, Bülbül M (September 2021). "Spondylenchondrodysplasia mimicking a systemic lupus erythematosus: A diagnostic challenge in a pediatric patient". European Journal of Medical Genetics. 64 (9): 104286. doi:10.1016/j.ejmg.2021.104286. PMID 34245909.
- ^ Bhargava R, Leonard NJ, Chan AK, Spranger J (June 2005). "Autosomal dominant inheritance of spondyloenchondrodysplasia". American Journal of Medical Genetics. Part A. 135 (3): 282–288. doi:10.1002/ajmg.a.30732. PMID 15887273. S2CID 31820771.
- ^ Frydman, M., Preminger-Shapiro, R., Bar-Ziv, J. Spondylometaphyseal dysplasia with 'enchondromatous-like' changes--a distinctive type. (Abstract) 7th International Congress of Human Genetics, Berlin 1986. Pp. 257-258.
- ^ de Bruin C, Orbak Z, Andrew M, Hwa V, Dauber A (2016). "Severe Short Stature in Two Siblings as the Presenting Sign of ACP5 Deficiency". Hormone Research in Paediatrics. 85 (5): 358–362. doi:10.1159/000443684. PMC 4891295. PMID 26789720.
- ^ a b Kulkarni ML, Baskar K, Kulkarni PM (January 2007). "A syndrome of immunodeficiency, autoimmunity, and spondylometaphyseal dysplasia". American Journal of Medical Genetics. Part A. 143A (1): 69–75. doi:10.1002/ajmg.a.31526. PMID 17163538. S2CID 20137648.
- ^ Schorr S, Legum C, Ochshorn M (January 1976). "Spondyloenchondrodysplasia. Enchondromatomosis with severe platyspondyly in two brothers". Radiology. 118 (1): 133–139. doi:10.1148/118.1.133. PMID 1244645.
- ^ Menger H, Kruse K, Spranger J (February 1989). "Spondyloenchondrodysplasia". Journal of Medical Genetics. 26 (2): 93–99. doi:10.1136/jmg.26.2.93. PMC 1015557. PMID 2918547.
- ^ Uhlmann D, Rupprecht E, Keller E, Hörmann D (August 1998). "Spondyloenchondrodysplasia: several phenotypes--the same syndrome". Pediatric Radiology. 28 (8): 617–621. doi:10.1007/s002470050431. PMID 9716637. S2CID 28521080.
- ^ a b c d e f Girschick H, Wolf C, Morbach H, Hertzberg C, Lee-Kirsch MA (September 2015). "Severe immune dysregulation with neurological impairment and minor bone changes in a child with spondyloenchondrodysplasia due to two novel mutations in the ACP5 gene". Pediatric Rheumatology Online Journal. 13 (1): 37. doi:10.1186/s12969-015-0035-7. PMC 4562156. PMID 26346816.
- ^ Lausch E, Janecke A, Bros M, Trojandt S, Alanay Y, De Laet C, et al. (February 2011). "Genetic deficiency of tartrate-resistant acid phosphatase associated with skeletal dysplasia, cerebral calcifications and autoimmunity". Nature Genetics. 43 (2): 132–137. doi:10.1038/ng.749. PMID 21217752. S2CID 205357235.
- ^ Gelen SA, Kara B, Şimsek IE, Güngör M, Zengin E, Sarper N (2021-11-02). "Autoimmune Hemolytic Anemia Due to Spondyloenchondrodysplasia with Spastic Paraparesis and Intracranial Calcification due to Mutation in ACP5". Journal of Pediatric Genetics. doi:10.1055/s-0041-1736560. ISSN 2146-4596. PMC 10984710. S2CID 243488478.
- ^ a b c Briggs TA, Rice GI, Daly S, Urquhart J, Gornall H, Bader-Meunier B, et al. (February 2011). "Tartrate-resistant acid phosphatase deficiency causes a bone dysplasia with autoimmunity and a type I interferon expression signature". Nature Genetics. 43 (2): 127–131. doi:10.1038/ng.748. PMC 3030921. PMID 21217755.
- ^ Le Merrer M, Fressinger P, Maroteaux P (July 1991). "Genochondromatosis". Journal of Medical Genetics. 28 (7): 485–489. doi:10.1136/jmg.28.7.485. PMC 1016962. PMID 1895320. S2CID 220169910.
- ^ Silve C, Jüppner H (September 2006). "Ollier disease". Orphanet Journal of Rare Diseases. 1 (1): 37. doi:10.1186/1750-1172-1-37. PMC 1592482. PMID 16995932.
- ^ Zack P, Beighton P (February 1995). "Spondyloenchondromatosis: syndromic identity and evolution of the phenotype". American Journal of Medical Genetics. 55 (4): 478–482. doi:10.1002/ajmg.1320550417. PMID 7762590.
- ^ a b Freisinger P, Finidori G, Maroteaux P (February 1993). "Dysspondylochondromatosis". American Journal of Medical Genetics. 45 (4): 460–464. doi:10.1002/ajmg.1320450413. PMID 8465851.
- ^ a b "Ollier Disease". NORD (National Organization for Rare Disorders). Retrieved 2022-10-23.
- ^ Jacob P, Bhavani GS, Shah H, Galada C, Nampoothiri S, Kamath N, et al. (March 2022). "Pseudoachondroplasia: Phenotype and genotype in 11 Indian patients". American Journal of Medical Genetics. Part A. 188 (3): 751–759. doi:10.1002/ajmg.a.62566. PMID 34750995. S2CID 243863457.
- ^ Tüysüz B, Arapoglu M, Ungür S (July 2004). "Spondyloenchondrodysplasia: clinical variability in three cases". American Journal of Medical Genetics. Part A. 128A (2): 185–189. doi:10.1002/ajmg.a.30078. PMID 15214014. S2CID 21547142.
- ^ Shimizu M, Inoue N, Mizuta M, Irabu H, Okajima M, Honda Y, et al. (February 2021). "Successful treatment of spondyloenchondrodysplasia with baricitinib". Rheumatology. 60 (2). Oxford, England: e44–e46. doi:10.1093/rheumatology/keaa356. PMID 32856090.
- ^ "Entry - #607944 - Spondyloenchondroplasia with immune dysregulation; SPENCDI - OMIM". www.omim.org. Retrieved 2022-10-23.
- ^ a b c Roifman CM, Melamed I (June 2003). "A novel syndrome of combined immunodeficiency, autoimmunity and spondylometaphyseal dysplasia". Clinical Genetics. 63 (6): 522–529. doi:10.1034/j.1399-0004.2003.00033.x. PMID 12786759. S2CID 41818818.