The intertrochanteric line is a line upon the anterior aspect of the proximal end of the femur,[1] extending between the lesser trochanter and the greater trochanter. It is a rough, variable ridge.[citation needed]
| Intertrochanteric line | |
|---|---|
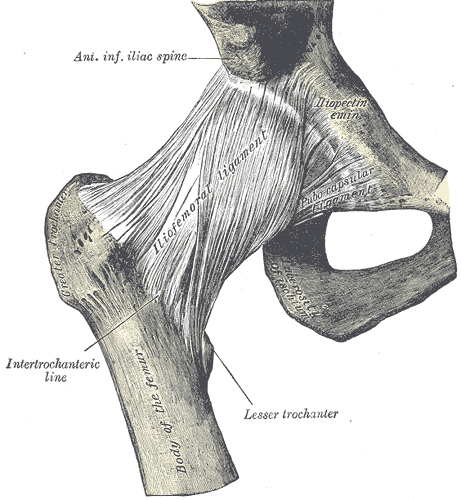 Right hip-joint from the front. (Intertrochanteric line labeled at bottom left.) | |
 Right femur. Anterior surface. (Intertrochanteric line visible near top, as diagonal line below neck.) | |
| Details | |
| Identifiers | |
| Latin | linea intertrochanterica |
| TA98 | A02.5.04.009 |
| TA2 | 1368 |
| FMA | 74587 |
| Anatomical terms of bone | |
Structure
editThe intertrochanteric line marks the boundary between the femoral neck and shaft anteriorly (whereas the intertrochanteric crest marks the same boundary posteriorly).[2]
Attachments
editThe iliofemoral ligament — the largest ligament of the human body — attaches above the line.[3] The lower half, less prominent than the upper half, gives origin to the upper part of the vastus medialis.[clarification needed][citation needed]
The distal capsular attachment on the femur follows the shape of the irregular rim between the head and the neck. As a consequence, the capsule of the hip joint attaches in the region of the intertrochanteric line on the anterior side, but a finger away from the intertrochanteric crest on the posterior side of the head.[4]
The fibers of the ischiocapsular ligament attach both into the joint capsule and onto the intertrochanteric line.
Clinical significance
editIntertrochantric fractures
editThis area of the femur being an important pillar for weight bearing through the skeletal system is subject to comparatively high levels of dynamic stress, pathological strain, physiological strain and trauma. This area is prone to fractures due to high velocity trauma in the young and trivial trauma in the elderly. The fractures in this line are called intertrochantric fractures and are classified as per the pattern of the fracture geometry.
After a fracture this area of bone is notorious for uniting in varying, and sometimes problematic angles. Therefore, it typically requires early surgical reduction and fixation with early mobilization and weight bearing in order to facilitate enhanced recovery.
References
edit This article incorporates text in the public domain from page 245 of the 20th edition of Gray's Anatomy (1918)
- ^ White, Tim D.; Folkens, Pieter Arend (2005-11-08). The Human Bone Manual. Elsevier. ISBN 978-0-08-048899-8.
- ^ Platzer (2004), p 192
- ^ White (2005), p 256
- ^ Platzer (2004), pp 192, 198
Bibliography
edit- Platzer, Werner (2004). Color Atlas of Human Anatomy, Vol 1: Locomotor system (5th ed.). Thieme. ISBN 3-13-533305-1. (ISBN for the Americas 1-58890-159-9.)
- Timothy D., White; Pieter A. Folkens (2005). The Human Bone Manual. Academic Press. ISBN 0-12-088467-4. Retrieved 2008-10-11.
External links
edit- Anatomy figure: 17:01-07 at Human Anatomy Online, SUNY Downstate Medical Center
- lljoints at The Anatomy Lesson by Wesley Norman (Georgetown University) (hipjointanterior)